Pain is an enigmatic concept. It is obscurely wrapped up in an intricate web of perceptions, emotions, memories, cognition and social interaction. It is also accompanied by experiences of anxiety, desperation and shame that many people overlook.
This installation was created from my perspective as an artist who has been living with painful conditions – endometriosis and adenomyosis– for all of my adult life.
Its genesis occurred when I came across an iconic objective pain assessment tool, the McGill Pain Questionnaire at a university library. I became elated with hopes that this questionnaire could be the ultimate validation tool that I had been searching for. I was fascinated by the incredible assessment methodology which finally acknowledged one’s subjective experience rather than addressing a human being as a biomechanical machine.
I have always been interested in exploring the objective and subjective dichotomy within the concept of art and pain science, so I immediately became curious about what artwork would look like if I combined this objective pain measuring tool with my subjective lived experience as a self-portrait installation.

MDF, motor, barbed wire, timber, perspex, paint, handles, label holders, paper, TV screens, DVD players, fluorescent light
360x200x50 cm
Installation view: Main Gallery, Sydney College of the Arts, University of Sydney 2012
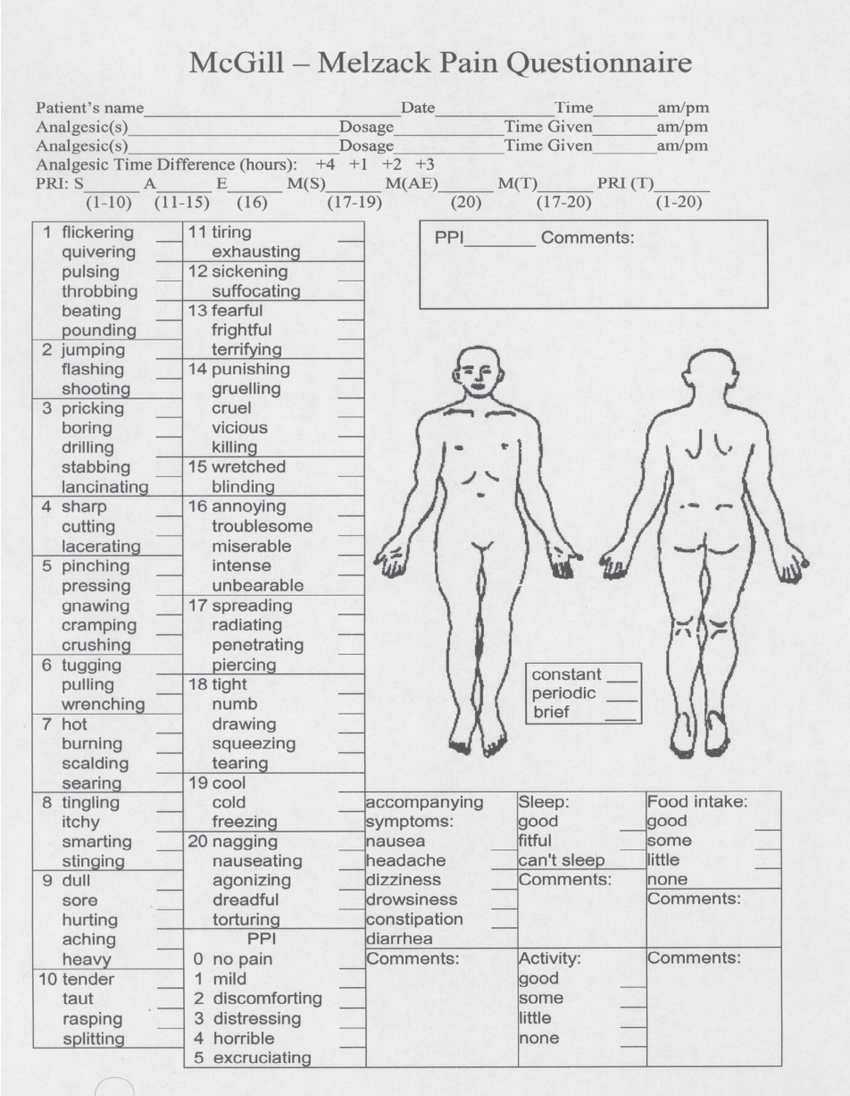
What is the McGill Pain Questionnaire?
The McGill Pain Questionnaire, developed in the 1970s by two psychologists, Dr Ronald Melzack and Dr Warren Torgerson, changed the way that the medical system measured pain.
It is essentially composed of a list of seventy-eight descriptive similes that are used as a clinical pain assessment tool. The method is intended to give a person the ability to communicate their pain to their physicians, and the shorter form is still used as a mediator for pain in the field of current medicine. Once thought unmeasurable, this questionnaire became an important and influential tool for other pain measurement questionnaires. To a limited degree, it enables subjective experiences to be objectified and presents a partial insight into certain characteristics of an individual’s pain. The questionnaire acknowledges and examines the multi-dimensionality of pain rather than simplifying it wholly into the quantitative intensity of pain – that is, measuring the severity of pain based solely on numerical values from 0 to 10. It all sounds good in theory, but the original questionnaire is rather complicated to use in practice.
Although I will not go into the technical details of its methodology, the questionnaire remains a ground-breaking achievement as it provided much-needed opportunities for pain patients to coherently express their experiences. Some of the selected words from the questionnaire have since become an important language tool for clinical diagnosis. A few adjectives brought up by a patient could give the physician a better chance of determining an appropriate treatment to improve the life of the person in pain. Through this remarkable finding of the consistency of verbal descriptors, pain has become more communicable and also better measured, recorded, and referenced. The McGill Pain questionnaire is not perfect. It does not capture complex pain-related issues, but in its day, it was an important step forward in the analysis of pain from the patient’s perspective.

Installation view: Art of Pain, curated by Vicki Sowry (ANAT), Kerry Packer Civic Gallery, The Hawke Centre, Samstag Building, University of South Australia 2015
Filing Cabinets: furniture that both stores and transforms one’s personal experience into a reliable and orderly structure
My artwork, McGill Pain Questionnaire, incorporates filing cabinets as an agency to systematically organise and externalise subjective pain experiences. The idea was drawn from The Poetics of Space,[1] in which Gaston Bachelard asserts that various architectural structures that deal with inside and outside, such as wardrobes and cabinets, are metaphors for the complex human psyche. Our intimate ideas, memories, thoughts and feelings are stored and organised inside these constructions.[2] He states that once these ideas have been objectively archived, there is no longer any need to rely on inconsistent memories, as they are replaced by a reliable filing system.[3] In my installation, I use these features of filing cabinets to represent how the medical system clinically catalogues and attempts to organise the private experiences of people in pain. The cabinets are also a surrogate for the pained body and psyche living within the seemingly perfectly functioning façade of a person.
McGill Pain Questionnaire takes the form of two large filing cabinets narrowly facing each other, between which viewers stand. Monotonous drawers cover the faces of both cabinets, labelled with all the adjectives contained in the questionnaire and following its ‘as if/as though’ pain descriptor methodology. The symmetrical and uniformly organised façade of the filing cabinet contrasts with the overwhelming lack of control felt when a person begins to experience body disownership.

Installation view: Art of Pain, curated by Vicki Sowry (ANAT), Kerry Packer Civic Gallery, The Hawke Centre, Samstag Building, University of South Australia 2015
The labels are placed at random to defy the questionnaire’s attempts to enforce order and strictly systemise the sum of our experiences within its seventy-eight adjectives and twenty sub-groups. To augment the adjectives of the pain descriptions of the questionnaire, I incorporated visual metaphors and similes into the installation in the form of viewing windows. The moving images within viewing windows on both sides show selected visual manifestations of my persistent pain.
How do we measure pain, which encompasses all aspects of our lives, on a piece of paper with a limited range of words? Like many people living with long term pain, I have struggled with a sense of loss, existential crisis, and a destroyed sense of agency.

Installation view (detail)
Pain is invisible. Proving it even exists is difficult – it doesn’t show up on a scan and there is no hard evidence of its presence. Communicating about pain is also problematic, it relies on the verbal accounts of the people who experience it, but these accounts are not always believed. So how do we navigate through these barriers?
The installation explores these tricky issues – expressions and invisibility. There is no adequate substitute for one’s pain perception itself which can never be fully shown nor conveyed directly or be truly validated through words.
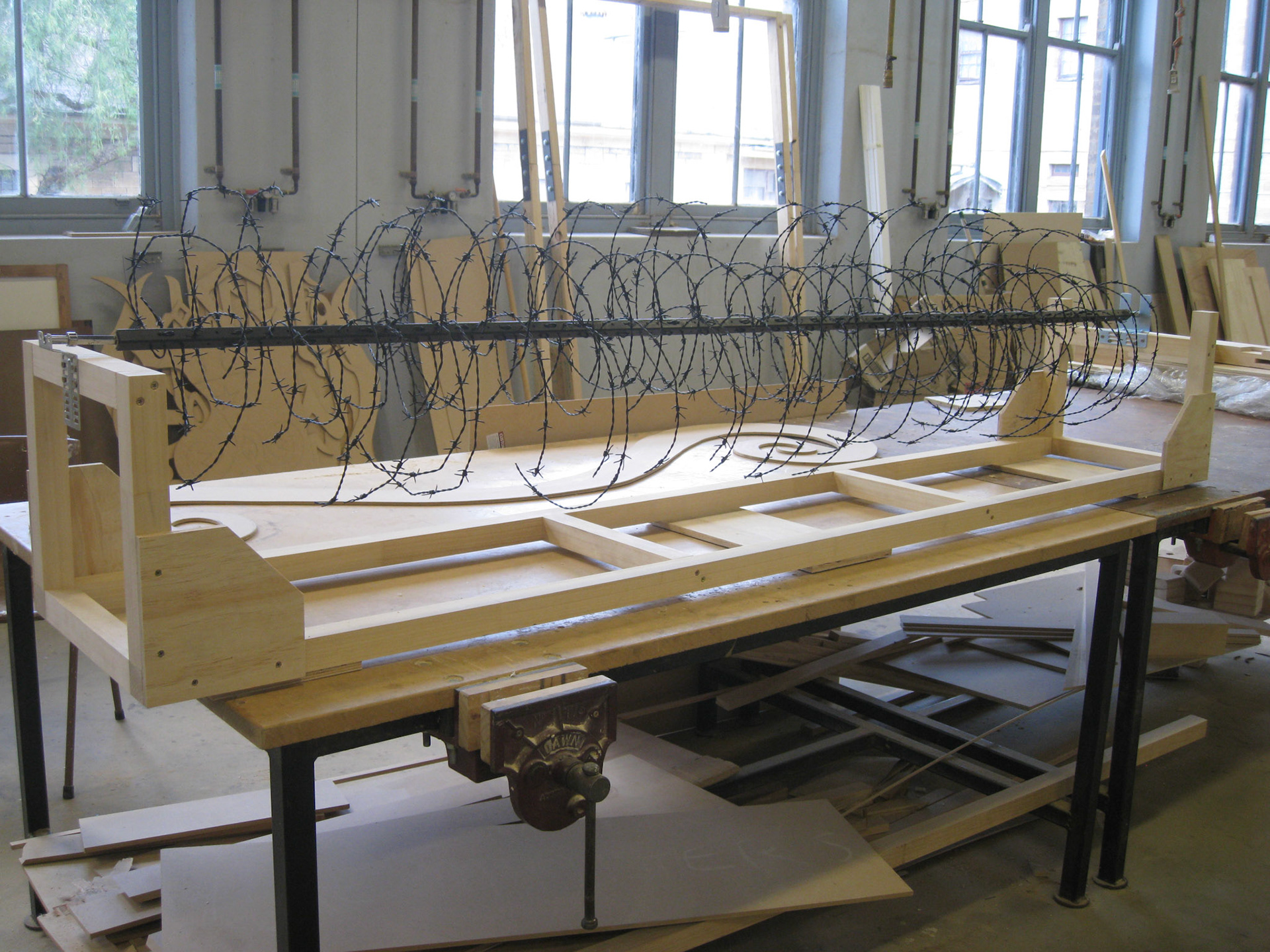
The long viewing window on one side of the cabinet shows a particular simile that I have often used to describe my visceral pain: “it feels like strings of barbed wire are scraping against my organs”.
To visually implement this effect, I employed barbed wire attached to a mechanism behind the viewing window. As the barbed wire rotates, it digs and tears the insides of the installation. Accompanying this is the eerie noise of scraping and gouging. The barbed wire slowly eats away the inner surface of the plexiglass whilst the outside texture maintains a seemingly unblemished smooth texture.
It symbolises an experience that is externally imperceptible, yet certainly exists for the person feeling it.

Installation view: Main Gallery, Sydney College of the Arts, University of Sydney 2012
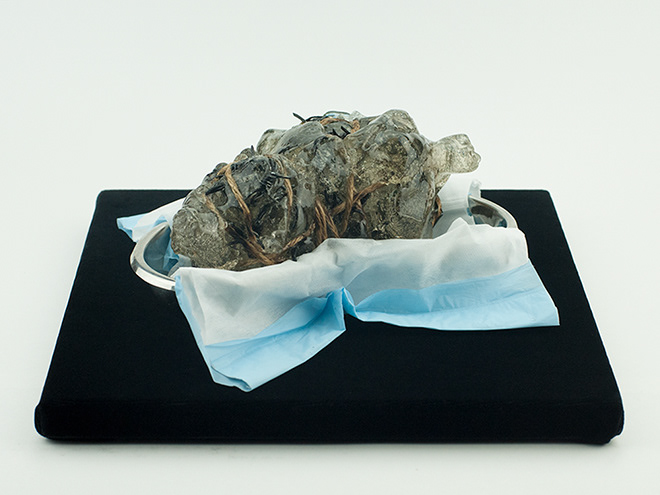
The opposite viewing windows show a selection of my other pain perceptions via three video screens: “it feels as if it is pulsing, shooting and stabbing inside me”. Each screen shows a visual interpretation of one of these three descriptors. The materials used to illustrate this experience are seaweed, ink, and thickened milk. When we are unwell, most of us tend to spend a lot of our time at home for protection and comfort but people often overlook the hidden threats within the idealised idea of home. I wanted to represent this ambiguous dichotomy by incorporating materials from my own kitchen where close social domestic interactions take place.


Growing up in South Korea I ate a lot of seaweed as it was a staple of the Korean diet. Although I now live in Australia, I still store plenty of seaweed in my pantry. Notwithstanding its health benefits, seaweed is sensitive to the well-being of its ocean environment. It absorbs everything, including toxic chemicals leaked into the ocean.
As my illness is affected by environmental and psychosocial factors such as dioxin as well as the quality of interactions with family and close network of people around me, I chose to employ seaweed as a metaphor for the bio-psycho-social influences.
Milk represents the hereditary factor of my illnesses and interrogates the generic healthy connotations of the material. Although clear causes are yet to be found, some research points towards strong links to the female line. My symptoms were also most highly active during the child-bearing years. Although milk is associated with birth, maternal love, and nurture, this is not necessarily a universal reality. Furthermore, in many cultures, dairy milk is collectively promoted as an essential food for the health of growing children. Like many, I am lactose intolerant and drinking it used to make me unwell, without understanding why.
I chose this material as a way of reclaiming a substance that physically and by association contributes to my illness. Interestingly, the latest advice for women living with endometriosis and adenomyosis is to avoid drinking milk.
Black food colouring, found in my kitchen, was used for its very quality of uncertainty – it often doesn’t produce consistent colour. Unlike the black paints I use for my paintings, over which I have full control, and which always meet my expectations, the food ink I used delivers unpredictable results, often different to what the manufacturer claims and for which they take no responsibility.
This parallels the lack of certainty with the result claims of the many unregulated treatment options that abound for under-researched medical conditions like mine. It is left up to the patient to take a leap of faith, to accept the claims of restored health and elimination of pain, without valid evidence nor consequence to the provider if those claims prove false.
Although the use of food colouring worked out in the end, the performative element of producing the videos with uncertain results, kept me in a constant state of anxiety.
Through the videos and the moving mechanism, I have tried to objectify the intangibility of my visceral experiences and to make sense of my private agony. I have embodied the structure of the filing cabinets to categorise my pain, whilst recognising the shortcomings of the questionnaire and my own attempt to convey something that is, by definition, incommunicable. Although pain is invisible, these windows, like medical scans, are the ‘evidence’ that my pain truly exists.
Whilst creating this self-portrait installation, I was deeply aware of the tension between the clinical system that is ultimately removed from its subject, and the human experience which has a history that is built and formed through layers of social interactions, emotions, and memories of lived experience. I wanted the viewers to reflect upon a sense of the individual being lost in medical discourse.
Definition of illness - Philosophy of Nature
Hegel describes an illness as a loss of vitality in an organism.[4] He states that illness can become assimilated into the life of the person living with it, making it necessary to treat the person as a whole, rather than focusing on the individual symptoms of illness.
According to Hegel, the presence of illness actively opposes the harmonious functioning of the body.[5] Yet, despite their illnesses, many complex organisms including humans manage to live with their obtrusive illnesses as an incorporated part of their life. Hegel calls the resulting loss of vitality from the diseased state an “irritation”[6], and argues that our body can still maintain its balance in the presence of irritation - for example, the excess of heat constituting fever - without being subject to the entire destruction of the body.[7] But when this equilibrium is overwhelmed by either excessive irritation or an inability to maintain the natural flow, the organism loses its balance. This can then lead to prolonged disease and potentially even death. The body can only return to a healthy state if an equilibrium is restored.
Chronic illness, as Hegel defines it, occurs when the system no longer has the ability to overcome the excessive irritation;[8] the body loses the capability to fight the disease and bring it back to a healthy state. Instead, the abnormality continues to stay isolated and imposes limitations on the activities of the entire body. The affected body, fluid and free in its healthy state, instead becomes fixed and dominated by the illness. The disease is no longer isolated inside a particular organ, nor acts as a separate being to the rest of the body. Because the organism has lost the ability to maintain its equilibrium by this stage, the abnormality extends its negativity towards the weakened centre of the whole body. The system is eventually consumed by the disease, which not only causes dysfunction but also becomes part of the general life of the individual person.[9]
This statement by Hegel implies a modern outlook, ahead of his time. In dealing with chronic illness, he suggests, all aspects associated with it must be taken into consideration, not just the visible elements of irritations, because it is not about the irritation anymore. Since the centre of a whole person is affected by the chronic illness, the treatment must therefore deal with this whole person rather than focusing on only the symptoms. A person as a sentient being is more than just a living body with anatomical composites. By taking into account mental and social factors as well as biomechanical, all matters towards chronic illness and pain must be considered to treat the whole person. Although Hegel’s scope of illness in Philosophy of Nature was limited to physiology,[10] his in-depth analogy of illness and how it affects our entire self parallels the current neuroscience of pain.
[4] Chapt 3C, section 3. Georg Wilhelm Friedrich Hegel, “Medical Science (The genius and the individual)”, Philosophy of nature, trans. M.J. Petry (Lond.: Allen and Unwin, 1970). 193-213.
[5] Hegel, Philosophy of Nature, 194-5.
[6] Ibid.
[7] Ibid.
[8] Ibid. 198.
[9] Hegel, Philosophy of Nature, 198
[10] Philosophy of Nature by Hegel was written in the early 19th century and it predates the understanding of the subjective aspect of pain.

L'homme de René Descartes (reproduced by permission of René Descartes Paris: Charles Angot, 1664)
One of the best-known historical pain theories is the seventeenth century Descartes’ pain pathway[11], which unfortunately is still viewed and taught as a valid mechanism of pain. In the drawing [Figure 1], an external influence such as fire (A) on a person’s foot (B) triggers a signal which travels through the leg (C), spine (D), and finally into the brain (F) to cause an alarm bell which the person then feels as pain. Descartes claimed it is much like the mechanism of a bell ringing in a church tower - a person pulls a rope near the ground, and the rope attached to the bell on the belfry makes it ring.[12]
Descartes’ pain analogy is purely based on the sensory mechanical aspect. It is a logical and causal description in that pain is seen as the direct result only of physical action or injury. Whilst this may be of use when studying acute pain, it is misleading when assessing the cause and effects of persistent pain.
The technical investigation of pain since Descartes’ era goes like this: the spinal cord acts as a bridge from the mechanics of the body to the pineal gland in the brain. Pain was believed to send noxious signals to the brain through the nerves in the spinal cord. Thus, in order to eliminate pain, all that was considered necessary was to either move the body part away from the noxious source or simply perform an excision of the associated nerve by surgery so that the sensory-processing brain can be disconnected from its cause and freed from the pain. Since the 1950s its conceptual medical theories and treatment of pain have undergone minor changes despite the emergence of new studies that show that the network of persistent illnesses and pain is much more complex than what was once believed.
Recent studies acknowledge the fact that pain is a subjective experience in which the perceptions and responses vary between individuals. Despite the fact that it is recognised that the perplexing structure of pain no longer corresponds solely to tissue damage, the centuries-old philosophical investigation by Descartes lingers stubbornly to this day as the dominant understanding of pain within our culture, and even within many areas of the medical sector. Current studies of pain discredit the Cartesian way of thinking about pain and instead advocate a two-pronged approach to treatment. According to these theories, biomedical science must be accompanied by a better understanding of the influences of cognitive, psychological, and social determinants – including the person’s past experiences, emotions, and social interaction. In these theories, pain is interpreted as a multi-dimensional ecosystem, incorporating one’s individuality and intersectionality.
Dennis Turk, a professor and researcher with a special interest in the assessment of pain, stresses that pain is not exclusively confined to the sensory experience; it cannot be presumed that all physical causes of persistent pain must either be detectable or characterised as psychiatric complaints.[13] Instead, Turk asserts, pain is an intense, individual experience of discomfort derived from complex composites of biological, psychological, and social phenomena. As a result of these views, it is now recommended that the objective and somatic view of the body in pain for medical treatment be replaced by a holistic approach; in other words, the body in pain is to be seen as a person in pain. However, despite these recent developments, the Cartesian dualistic outlook of pain - narrowly based on only the biomechanical aspect - is still accepted by many professionals in the field of medicine today. Furthermore, the intensity of pain, until recently, was the only facet to measuring the quality of the experience. The most used method was a quantitative measurement - ranging from 0 to 10, with 0 being no pain, to 10 being unbearable pain.
[11] Ronald Melzack & Patrick Wall (eds), The Challenge of Pain, (London: Penguin, 1988), 150.
[12] Ibid.
[13] D. C. Turk, "Chronic Pain: Models and Treatment Approaches," in International Encyclopedia of the Social & Behavioral Sciences, ed. Neil Smelser, J. and Paul B. Baltes,` (Oxford: Pergamon, 2001). Accessed May 24, 2012. Doi: 10.1016/B0-08-043076-7/03897-3.
The ‘unsharability’ of pain - The Body in Pain by Elaine Scarry
In The Body in Pain, Elaine Scarry describes the ways in which the medical field finds objective ways to measure and record pain. She claims that pain carries a peculiar dichotomy.[14] Because pain is experienced as an absolute and undoubtable agony for the person living with it, it can be seen as one of the fundamental definitions of certainty. Yet pain can also epitomise the very meaning of uncertainty for someone who does not feel it. The depth of someone else’s pain is difficult to grasp as an observer. There is often doubt in the mind of the person who is witnessing another’s pain, even if they are both in the same room. This very quality is what Scarry calls the “unsharability” of pain.[15] Because it is difficult to communicate pain through language, finding the precise words to convey a subjective and private agony is problematic. Scarry says pain resists the aid of language;[16] that the difficulty of expressing pain through words, whether physiological or psychological, is constantly in battle against a rudimentary scream or moan. However, there are ways to mediate this incommunicability via metaphorical descriptions and/or similes – ‘it feels like…’, ‘it feels as if …’.[17] These ‘as if’ sentences are often the most appropriate communication in language to express the pain experience. By presenting comparable connections through a metaphorical description, it gives pain material features like shape, weight, and colour. An example would be – “it feels like red hot coals are searing my knees.”
The same effect can be achieved through art and music; by transforming the original incommunicable and ineffable pain into an object or experience it becomes communicable to others.[18] Rather than pain being confined internally, art allows the private agony of pain to be externalised, and ultimately become sharable.[19]
[14] Elaine Scarry, The Body in Pain: The Making and Unmaking of the World (New York, Oxford: Oxford University Press, 1985), 4.
[15] Ibid.
[16] Ibid.
[17] Elaine Scarry, “The Poetics of Anesthesia”, in Pain and Its Transformations: The Interface of Biology and Culture, Sarah Coakley and Kay K. Shelemay, eds., (Cambridge, Massachusetts, London: Harvard University Press, 2007), 281-2.
[18] Ibid.
[19] Ibid. 282.

Installation view: Art of Pain, curated by Vicki Sowry (ANAT), Kerry Packer Civic Gallery, The Hawke Centre, Samstag Building, University of South Australia 2015
Conclusion
Pain affects most of us at some time in our lives in one way or another to varying degrees. It brings attention to the fact that we are not perfect, and that we are vulnerable. The experience of pain, either through illness or injury, is very much a part of our lived experience and is also a sign that we are alive.
The subjective nature of pain makes it difficult for a third party to understand its complexity. Pain is invisible, and directly trying to communicate this ambiguous yet fundamental perception can often add to the burden for the person living with it. The negative effects of illness span all aspects of our lives, not just the physical. In order to treat chronic illness and pain, it becomes necessary to address this multi-layered trait. Thus, Hegel’s position on the importance of treating a person with illness as a whole is still relevant today.
Fortunately, pain researchers in recent years have acknowledged the fact that each individual experiences pain differently. Perception of pain is no longer believed to be always symptomatic of a physiological disease or injury that can be located and seen. However, many aspects of pain still leave researchers and medical practitioners baffled, and it is even more difficult for the general public to understand its complex nature. I do not assert that the new theories and praxis of pain can answer all the challenges of communicating one’s pain – as is pointed out through the closed doors and smooth façade of the plexiglass in my installation.
I would like to see both patients and physicians equally present with curiosity and optimism for each pain experience, rather than seeing pain through the lens of the existing social stigma. This idea of collaboration is a surprising outcome of my installation, one I never consciously intended but that I now contemplate with the rhetorical question - what would it look like if we, as individual subjective emotional beings, could co-exist alongside objective medical science?
We are, as interrelated social beings, always by default trying to communicate with others – to connect, adapt, negotiate, and disrupt - even with the clinical façade of the impartial medical system, because behind that facade there are real people.
Amongst the unresponsive solid locked drawers in the installation, the viewing windows provide visual narratives laying bare some of the multifaceted visceral natures of the pain experience. These windows speak the ‘truth’ of one’s lived experience in a way no words could ever replace and are as valid a way of communicating as any scientific pain measurement tool, if not better. Creating these windows was my way of legitimising my experience that could resonate with others.
The collaboration focuses on drawing out the emotional connections between people, bypassing the hierarchical structures of the traditional physician and patient relationship.
There is room for art to fill in some of the gaps alongside science, as an alternative storytelling platform, and in allowing the audience to create meaningful relevance and connections with what is essentially an abstract concept. In fact, pain and art have something in common. They both benefit from using metaphorical, visual, and experiential forms to better communicate and share concepts with others. Through this work, I hope to generate a better understanding of the complexities of pain for myself and for the wider audience.